 |
||||||
| home | learn about your condition | about somatics | site contents | store | testimonials | contact Lawrence Gold |
|
|
|||||||||||||||||||||


|
Common TMJ CausesTMD Syndrome/Bruxism/
|
|
TOPICS |
|
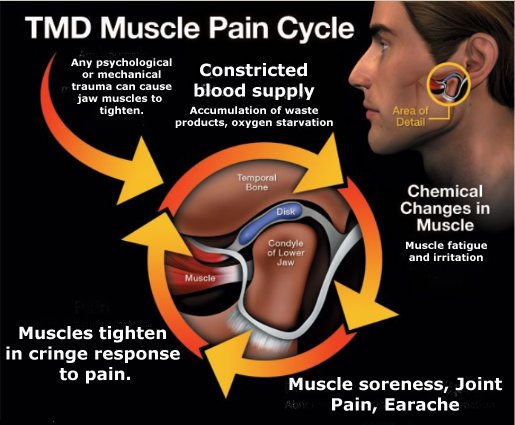
Dentists commonly regard TMD as being of different types: joint arthritis at the temporo-mandibular joint (TMJ), muscular soreness (myalgia), articular disc displacement, misfit of the upper and lower jaws, or of traumatic origin. However, all of these conditions reduce down to the same cause: overactive muscles of biting and chewing, so the same kind of treatment relieves them all (except for "disc displacement without reduction", which is a surgical situation). Let's see how. |
||
Degenerative ArthritisDegenerative arthritis of the TMJ does not just "happen by itself" (from genetics).It results from excessive compression forces upon the TMJ, imposed by chronically tight muscles of biting and chewing. The joint breaks down under pressure. To be effective, treatment must retrain those muscles out of clenching to a normal, low tension resting state (with "float space" between teeth). |
|
|
Muscular SorenessChronically tight muscles get sore. This soreness is the ordinary burn of muscle fatigue.Once muscles relax, the "burn" disappears in 30 to 90 seconds. For a lasting reduction of muscle tension and soreness, muscles must return to rest at a healthy, low tension level. Massage, stretching, splints and mouthguards are inefficient at retraining those muscles' tension level; however, an efficient training process does exist, to be discussed, later.
When jaw muscles are chronically tight, the articular disc gets squeezed between the two surfaces, upper and lower, and may get dragged out of place by jaw movements (displacement) -- a very painful condition.
If the displacement is within the rebound capacity of the attaching ligament, the disc can return to its home position ("disc displacement with reduction"), once excessive compression forces ease. If the ligament gets stretched past its rebound capacity, the disc stays out of place ("disc displacement without reduction").
While something radical like surgery may seem to be necessary, it's sufficient is to free the jaw muscles from clenching. With "float space" between the teeth comes tolerance of the mismatched situation to the point where it is comfortable. |
||
Conditioning InfluencesThe jaw muscles, like all the the muscles of the body, are subject to conditioned muscular reflexes that affect chewing and biting movements. The reason you don't go around slack-jawed and drooling, for example, is that a conditioned postural reflex causes the muscles of biting and chewing always to remain slightly tense, keeping your jaws closed.People's jaw muscles are always more or less tense, even when they are asleep. The norm is for your muscles of biting and chewing to be very mildly tense -- just enough to keep your mouth closed and lips together, but easy to open. The degree of tension you hold is a matter of conditioning. For brevity, I'll discuss only conditions that lead to TMJ/bruxism and not the normal development of muscle tone in the muscles of biting and chewing. These influences fall into two categories:
Emotional StressEver heard the expressions, "Bite your tongue"? "Grit Your Teeth"? "Bite the Bullet"? "Hold your tongue"? "Bite the Big One"? They all have something in common, don't they? What is that?To someone who regularly represses emotion or the urge to say something, these expressions have literal meaning. Emotional suppression or repression shows up as an involuntary grimace that includes clenching and pulling back the lower jaw. More on that here.
Such repression, over time, manifests as tension held in the muscles of speech -- in the jaws, mouth, neck, face, and back -- the same as the muscles of biting and chewing.
Although people experience trauma to the jaws through a fall, blow, or motor vehicle accidents (whiplash injury to the neck), the most common form of physical trauma (other than dental disease) is dentistry, itself, and it's unavoidable. Dental surgery is traumatic. The relevant term is "iatrogenic" -- which means "caused as a side-effect of treatment". Every dental procedure (and every surgical procedure) should be followed by a process for dispeling the reflexive guarding (cringe response) triggered by the procedure. (See the video.) No doubt, this assertion will distress dentists, and as much as I regret that, how can we escape that conclusion? It's obvious, isn't it? Consider the experience of dentistry, both during and after dental surgery (fillings, root canal work, implants, cosmetic dentistry, crown installation, injections of anaesthetic, even routine cleanings and examinations -- notice how a mere mention of those procedures makes you want to cringe). Consider the response you have to that kind of pain or even the expectation of pain: you cringe, don't you? We may think such cringing to be momentary, but consider the intensity of dental surgery; it leaves intense memory impressions on the nervous system evident as patterns of tension. (Who's relaxed going to the dentist? -- or coming out of the dentist's office?) The physical after-effects show up as tension in the jaws and neck, often in the spinal musculature -- and as a host of other symptoms. Let's go back to our memories of dentistry. If you've observed your physical reactions in the dentist's surgery station, you may have noticed that during probing of a tooth for decay (with that sharp, hooked probe they use), you tighten not just your jaw (can you feel it?) and your neck muscles (can you feel it?), but also the muscles of breathing, your hands, and even your legs. It's an effort to remain lying down in the surgery station when, bodily and emotionally, you want to get up and get out of the dentist's office. With procedures such as fillings, root canal surgery, implants and crown installations, the muscular responses are more specific and more intense. For teeth near the back of the jaws, we tense the muscles nearer the back of our neck; for teeth near the front of the jaws, we tense the muscles closer the front of the throat, floor of the mouth and tongue. This reflexive response has a name: Trauma Reflex. Trauma Reflex is the universal, involuntary response to pain and to expectation of pain. It gets triggered in relation to the location of the pain and to our position at the time of pain. Muscular tensions form as an action of withdrawing, avoiding, or escaping the source of pain. In dentistry, with the head commonly turned to one side, in addition to the simple trauma reflex associated with pain, we have the involvement of our sense of position, and not just the muscles of the jaws are involved, but also those of the neck, shoulders, spine. All of these conditions combine into an experience that goes into memory with such intensity that it modifies or entirely displaces our sense of normal movement and position. We forget free movement and instead become habituated or adapted to the memory of the trauma (whether of dental work or of some other trauma involving teeth or jaws). Our neuro-muscular system acts as if the trauma is still happening, even though, to our conscious minds, it is long past, and the way it acts as if the trauma is still happening is by tightening the muscles that close the jaws. Since accidents and surgeries address teeth at one side of the jaws or the other, the tensions occur on one side of the jaws or the other. Thus, the symptoms of such tension -- jaw pain, bite deviations, and earaches -- tend to be one-sided or to exist on one side more than on the other. The proof of the role of trauma reflex? -- the permanent changes of bite and tension of the muscles of biting that have behind them a history of dental trauma -- and the changes you see in the video that occur as this man is relieved of those conditioned postural reflexes. View the video and see for yourself.
|
|
Get started for free with a self-relief program
Point and click, TMJ Pain Treatment
|
|
The Institute for Somatic Study and Development
Lawrence Gold, C.H.S.E.
|
